
AI Scribe for Therapists: How Automated Notes Save Hours Each Week
Outline
The average outpatient therapist spends three to four hours per week writing progress notes. At 50 minutes per session, that’s one full session slot every working day spent on documentation that no client is present for. An AI scribe for therapists works by generating structured notes from session content, reducing that time to a review-and-edit task rather than a writing task. The newer therapy-specific tools go a step further: instead of passively transcribing what was said, they assist actively in the room, surfacing pattern signals, suggested interventions, and next-step prompts that connect to the client’s treatment plan.
This guide covers what AI scribes actually do in practice, how they handle SOAP, BIRP, and DAP formats, what HIPAA compliance looks like for session recording, and where the genuine limitations are.
If you are deciding whether note automation is enough, the AI co-therapy vs AI scribes comparison explains where a scribe-only workflow ends and where active co-therapy begins.
What an AI scribe for therapists actually does
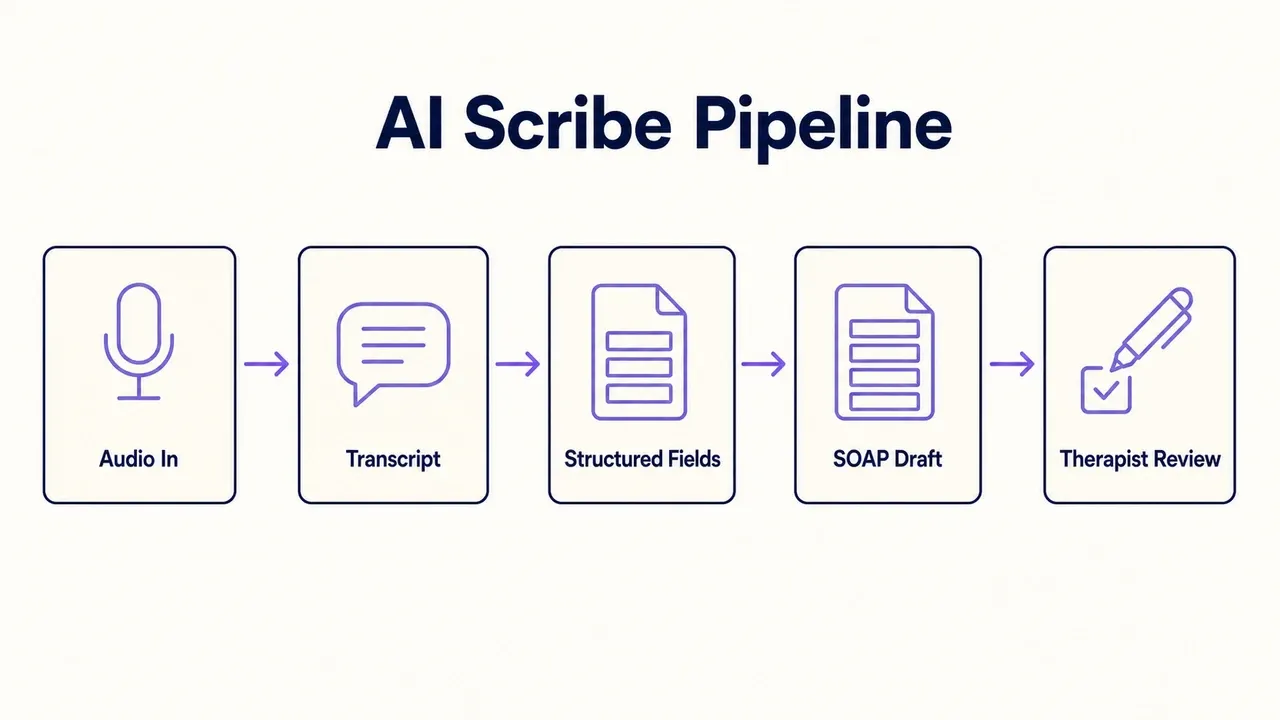
An AI scribe listens to or reads a session transcript and produces a structured note draft in whichever format you use — most commonly SOAP, BIRP, or DAP. You review the draft, edit for clinical accuracy, and sign off. The AI doesn’t make clinical judgments; it organizes what was said into the sections your note format requires.
In practice, this changes the workflow from:
- Finish session
- Reconstruct what happened from memory
- Write the full note
- Review and sign
To:
- Finish session
- Review AI draft with session still fresh
- Edit and sign
The second workflow is faster and more accurate — notes written immediately after a session while reviewing a draft capture more detail than notes reconstructed from memory at the end of the day.
SOAP, BIRP, and DAP: how format generation works
Each note format structures the same session content differently, and AI scribes handle all three.
SOAP (Subjective, Objective, Assessment, Plan) separates what the client reported from what you observed, then adds your clinical interpretation and next steps. It’s the most common format in outpatient mental health and the one most payers expect.
BIRP (Behavior, Intervention, Response, Plan) foregrounds what you did and how the client responded — a better fit for settings where skills training or behavioral rehearsal happens every session.
DAP (Data, Assessment, Plan) collapses Subjective and Objective into a single Data section. Useful when the distinction between client-reported and clinician-observed data matters less, as in case management.
AI scribes generate whichever format you set as default. The draft puts the right content in the right section; your job is to check that the clinical interpretation is accurate rather than assembling the structure from scratch.
HIPAA compliance and session recording
The most common question therapists have before using an AI scribe isn’t about note quality — it’s about privacy. Whether you’re recording sessions or uploading transcripts, HIPAA’s requirements are clear: you need a signed Business Associate Agreement (BAA) with any vendor who handles protected health information.
What to look for before using any AI scribe:
- Signed BAA available (not just promised — request it before starting)
- AES-256 encryption for data at rest and in transit
- Clear data retention policy, including deletion on request
- No training of AI models on client session content by default
- Audit logs showing who accessed records and when
Informed consent from clients is also required before recording any session. This is separate from your standard consent form — clients need to understand specifically that sessions may be processed by a third-party AI system, and they have the right to decline. Some clients will decline, and that’s a legitimate choice. For those clients, the workflow reverts to manual note-writing; the tool doesn’t need to apply to every client to be worth using.
For a detailed overview of HIPAA requirements in AI-assisted clinical work, see our guide on navigating HIPAA regulations for AI therapy.
Time savings: what the research shows
A systematic review of EHR documentation found clinicians spending up to 49% of their working time on administrative tasks rather than direct client contact (Baumann et al., 2018). AI scribes reduce that burden: outpatient practices using ambient scribes consistently report documentation time dropping by 30–50%, with mental health settings toward the lower end because the Assessment and Plan sections require clinical interpretation that the AI can draft but not finalize. A realistic expectation for a full therapy caseload is 30–45 minutes returned per session day.
For a full caseload of 25–30 sessions per week, that’s 2–3 hours per week returned to clinical work, supervision, or simply leaving the office at a reasonable time.
EHR integration
AI scribes fit into most practices in one of two ways: as standalone tools you export notes from, or as direct integrations with your practice management platform. Common integration points include SimplePractice, TherapyNotes, and Jane App. The workflow typically involves:
- Uploading or transcribing the session in the AI scribe tool
- Reviewing and finalizing the note draft
- Exporting or syncing the completed note to your EHR
Platforms that connect directly to your EHR eliminate a copy-paste step and reduce the chance of notes being saved in non-compliant locations (local drives, email drafts, unencrypted apps). If your current platform doesn’t offer direct integration, check whether the AI scribe exports in a format your EHR can import.
Limitations worth knowing before you start
AI scribes work well for structured progress notes in predictable session formats. They are less reliable in:
- Crisis sessions: High-acuity content with rapid clinical decisions doesn’t map cleanly onto standard note sections. AI-generated drafts for crisis sessions require heavier editing and should be treated with extra care.
- Sessions involving minors: Documentation requirements differ, and AI systems trained on adult therapy sessions may produce drafts that miss key elements (parent/guardian contact, school coordination, mandatory reporting considerations).
- Court-ordered or forensic contexts: Documentation here carries legal weight that requires explicit clinical authorship. AI-generated drafts are a liability risk, not a time-saver.
- Highly relational or process-oriented modalities: EMDR reprocessing sessions, IFS parts work, or somatic sessions don’t always produce the kind of verbal content that AI scribes convert well. In these cases, the draft often requires more editing than it saves.
When a generic AI medical scribe is the wrong tool for therapy
Most of the AI scribes on the market today were built for primary-care visits, urgent-care rooms, and hospital discharge summaries. Heidi, Nuance DAX, Suki, Abridge, and Freed all target physicians as the primary buyer. They work well for that workflow. The friction shows up when therapists try to use them for talk-based therapy. We map this out in detail in our Heidi alternatives for therapists comparison.
A therapy-specific tool and a general medical scribe are not interchangeable. The two were designed against different clinical workflows, and the differences accumulate across a full caseload:
| Capability | General AI medical scribe | Therapy-specific AI tool |
|---|---|---|
| Note format support | SOAP only, structured for medical encounters | SOAP, DAP, BIRP, and GIRP, the formats therapy practices actually use |
| Modality awareness | Generic medical Assessment section | Frames notes around CBT, ACT, DBT, EMDR, and IFS work |
| Treatment-plan continuity | Each session is a standalone artefact | Notes link to treatment plan goals and outcome measures across sessions |
| In-session role | Passive transcription | Surfaces patterns, suggested interventions, and next-step prompts during the session |
| HIPAA framing | Hospital and clinic workflow | Distinguishes psychotherapy notes from progress notes per HIPAA § 164.501 |
| Therapeutic-alliance signals | Not surfaced in the draft | Pattern detection across sessions feeds into formulation |
The four scenarios where the mismatch becomes a real problem:
- Modality-driven sessions. A general scribe that doesn’t recognise an ACT defusion exercise or an IFS parts dialogue produces a draft Assessment that misses the clinical content of the session. Editing that draft takes longer than writing from scratch.
- Between-session continuity. Therapy is a longitudinal relationship, not a series of independent encounters. A scribe that treats each session as a standalone visit doesn’t carry the thread from intake through phase 12.
- Note-format flexibility. SUD/IOP settings need BIRP or GIRP. A SOAP-only tool means the practice has to choose between using the scribe and using the format payers and supervisors expect.
- Therapy-specific HIPAA. The psychotherapy-notes carve-out (separate file, restricted disclosure, not part of the designated record set) doesn’t exist in primary care. A generic scribe that treats every artefact as a progress note creates a compliance gap. For a deeper look at this, see our HIPAA-compliant therapy notes workflow and the AI SOAP notes format guide.
This is the difference between a tool that documents your sessions and a tool that does therapy-shaped work alongside you.
How Emosapien handles AI-assisted documentation
Emosapien generates SOAP, DAP, and BIRP drafts from session content for therapist review, with a signed BAA, AES-256 encryption, and a policy of not training AI models on client data. Notes link directly to treatment plans and outcome measures so the clinical record stays connected across intake, sessions, and reviews.
How Emosapien is different from a scribe-only tool: documentation is one layer in a workflow that also covers intake, in-session support, between-session engagement, and outcomes. For the full comparison, see AI Co-Therapy vs AI Scribes.
Want a tool that does the documentation work during the session, not after it? Emosapien’s AI Clinical Notes drafts SOAP, DAP, and BIRP notes while you stay focused on the client. Therapy-shaped output, not generic medical scribing built for GPs and EMTs, with the modality-aware Assessment that mental health work actually needs.
Try Emosapien to see how AI-assisted note-writing fits into your current documentation workflow.
References
- Baumann LA, Baker J, Elshaug AG. The effect of electronic health record systems on clinical documentation times: A systematic review. Health Policy. 2018.
- U.S. Department of Health & Human Services, HIPAA Privacy and Security Rules
- HealthIT.gov — Electronic Health Records