Window of Tolerance Worksheet for Therapists
Outline
Authored by Dr. Elena Vasquez, licensed psychologist (PsyD), play-therapy and child-and-family-therapy trained, with a family-systems lens across home, school, and clinic.
A window of tolerance worksheet helps clients and therapists map the range where feeling, thinking, relating, and choosing are still possible. The form is not meant to make distress disappear. It gives the client, caregiver, and clinician shared language for noticing when the nervous system is moving toward hyperarousal, hypoarousal, or a workable middle range.
That distinction matters in trauma-aware work. A child may look oppositional when they are actually over the top of their range. A teen may look detached when they are below it. A caregiver may push for explanation right when the young person has lost access to language. The worksheet slows that loop down so the care team can respond to state before asking for insight.
This guide is written for therapists using the window of tolerance as a stabilization, pacing, and review tool with children, adolescents, families, and trauma-affected clients. It is not a stand-alone trauma protocol, a crisis plan, or a substitute for clinical judgment.
Where the worksheet fits clinically
The window-of-tolerance frame is most useful when the treatment task is state awareness and pacing. You are helping the client notice what their body, attention, voice, behavior, and relationships look like when they are in range, then identify the earliest signs that they are leaving that range.
It sits between broader therapy worksheets and more immediate stabilization tools. A grounding techniques worksheet usually answers, “What do I do right now to come back to the present?” A window map answers, “How do we recognize the state shift earlier, choose support sooner, and review what helped?”
For children and adolescents, the worksheet often belongs inside a family or school context. The client may not be the only person who needs the map. Caregivers, teachers, coaches, and other adults may need a simpler version of the same cues so they can reduce demands, offer co-regulation, and avoid escalating the moment.
The worksheet structure
A useful arousal-range worksheet should be visual enough to hold under stress and specific enough to guide a session review. Keep it to one page when possible.
The worksheet should not require the client to write a long explanation while dysregulated. Language often returns after regulation, not before it. Use the form to capture cues and supports first. Reflection can wait until the client is back within reach.
How to introduce the map
Start with normalization, not pathology. Children and teens often hear state language as another way adults are saying, “You are too much” or “You shut down.” The introduction needs to make clear that every nervous system has limits and that mapping limits is a way to protect agency.
With younger children, draw three zones with colors, weather, animals, or body shapes. With adolescents, ask permission before using language that may feel childish. Some teens prefer words like steady, overloaded, and offline. The clinical frame is the same. The dignity of the format changes whether they will use it.
Caregivers need their own introduction. A parent who sees the map only as a behavior-management tool may use it to correct the child, which defeats the purpose. Frame the caregiver role as noticing state, lowering unnecessary demand, and supporting return to range before problem-solving.
A child and caregiver example
The goal is not to force the child back to the worksheet. The goal is to help the adults recognize that the learning task has temporarily become a regulation task. Once the child is back in range, the family can decide whether to return to homework, shrink the assignment, or bring the pattern into therapy.
A teen example
Adolescents often need privacy and choice built into the map. A teen may be willing to identify lower-edge cues with a therapist but not want every cue sent to a caregiver or school. Respecting that boundary can make the difference between useful collaboration and surveillance.
That last question keeps the work relational. Regulation is not only about calming the body. It can also protect repair from happening too fast, too publicly, or from a state that the teen later regrets.
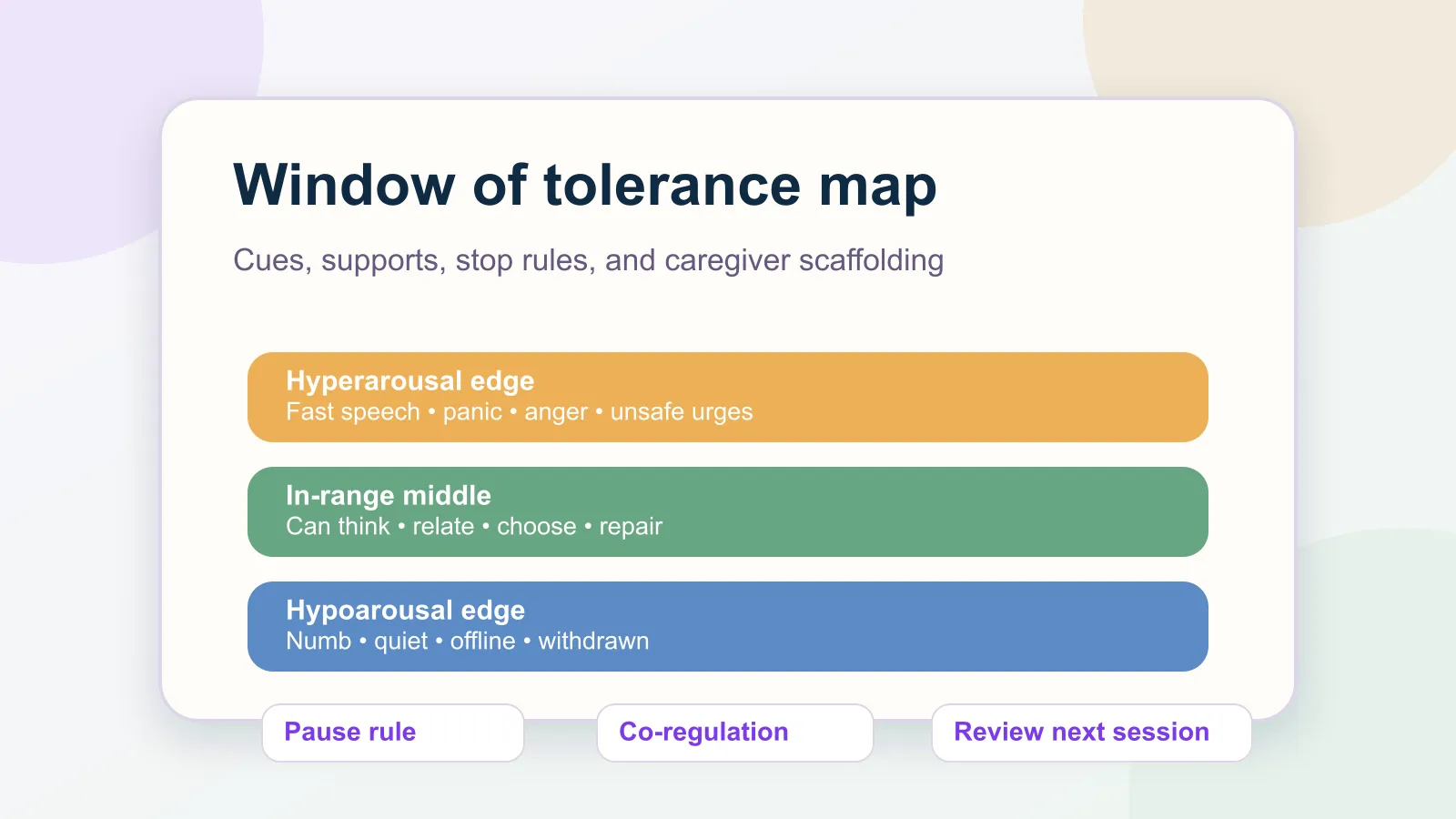
Hyperarousal, hypoarousal, and the middle range
Many clients recognize hyperarousal first because it is visible: anger, panic, rapid speech, agitation, argument, avoidance through action. Hypoarousal can be easier to miss. It may look like compliance, flat affect, fatigue, or indifference. In children, it can look like hiding, freezing, or sudden silliness that disconnects from the room.
A good window of tolerance worksheet makes both edges visible. If the map only tracks escalation, the quieter forms of shutdown stay invisible. If it only tracks shutdown, the client may miss the earlier agitation that came first.
For trauma-affected clients, body-based questions need pacing. Some clients can identify sensations with relief. Others become more activated when attention turns inward. If body scanning increases panic, shame, or dissociation, move back to observable cues: voice, posture, movement, gaze, pace, words, and interaction with the room.
How to use it between sessions
Between-session use should be small. “Track your window all week” is too broad for most clients. Choose one predictable transition or one recent pattern.
Examples:
- A caregiver notices the child’s upper-edge cues during the after-school hour on two days.
- A teen marks whether they were steady, overloaded, or offline after a known peer-stress moment.
- A family records one support that helped reduce conflict before bedtime.
- A client brings one example of a lower-edge cue that others usually miss.
The therapy check-in questions guide can help bring the worksheet back into session without turning review into interrogation. Ask what the client noticed, what support helped, what did not help, and what should be smaller next time.
If the client does not complete the form, treat that as information. The worksheet may be too long, too exposing, too verbal, too parent-driven, or too hard to access in the moment it was meant to support.
Documentation notes
Your progress note does not need to reproduce the full map. It should capture the intervention, the client’s response, and the plan clearly enough for continuity.
Document the clinically relevant pieces:
- state-awareness intervention used
- upper-edge or lower-edge cues identified
- caregiver or family-system role when relevant
- regulation support rehearsed or assigned
- stop rule or safety boundary
- next review plan
A concise note might read: “Introduced window-of-tolerance mapping to support trauma-informed pacing. Client identified upper-edge cues of fast speech and urge to leave room, and lower-edge cue of blank stare. Rehearsed caregiver co-regulation script and agreed to pause homework questions when lower-edge cues appear. Will review two after-school examples next session.”
That level of detail shows the clinical thread without turning the record into a copy of the worksheet.
Common mistakes
The first mistake is turning the map into a compliance chart. The window is not a way to label good and bad behavior. It is a shared clinical language for state, capacity, and support.
The second mistake is asking for trauma narrative too early. If the worksheet becomes a doorway into detailed recall before stabilization is in place, it has drifted from pacing to pressure.
The third mistake is ignoring hypoarousal. Some clients look calm when they are disconnected. The map should help you distinguish regulated quiet from shutdown.
The fourth mistake is leaving caregivers out when the client is a child. A young client may need the adult system to slow down before any self-regulation skill is reachable. Co-regulation is not an optional add-on. It is often the bridge.
Where Emosapien fits
A window of tolerance worksheet only helps if it comes back into the next clinical decision. Emosapien can help therapists turn one regulation map into a brief between-session check-in, bring back caregiver or client observations, and summarize the pattern before the appointment. The therapist still sets the pace, interprets the state cues, and decides what belongs in the plan.
For practices already using structured worksheets and AI clinical notes, the Engagement Agent and Scribe Agent can keep the map, review prompt, and documentation thread connected. Start for free and keep regulation work attached to the care relationship, not lost in a folder.
References
- National Child Traumatic Stress Network. (n.d.). Psychological First Aid Field Operations Guide. NCTSN.
- Substance Abuse and Mental Health Services Administration. (2014). Trauma-Informed Care in Behavioral Health Services, TIP 57. SAMHSA.
- Siegel, D. J. (1999). The developing mind: Toward a neurobiology of interpersonal experience. Guilford Press.
- American Psychological Association. (2017). Clinical Practice Guideline for the Treatment of PTSD. APA.