
Measurement Based Care in Psychotherapy: A Practical Guide for Busy Therapists
Outline
You already track so much in your head — changes in mood, shifts in risk, the way a client sits a little straighter when something clicks. Measurement based care (MBC) is about putting a small, structured frame around that intuition so you and your clients can see progress more clearly.
For many therapists, “measurement based care for therapists” brings to mind long questionnaires, extra paperwork and clients rolling their eyes at yet another form. It doesn’t have to look like that. With a few simple measures and a realistic workflow, MBC can support your clinical judgment instead of replacing it.
This guide keeps things practical: what MBC is, why it’s worth it, how to choose measures that fit your practice and how tools like Emosapien can make it sustainable.
What is Measurement Based Care (MBC)?
Plain Language Definition
Measurement based care just means using simple, repeated measures to inform therapy.
Instead of relying only on memory and impressions, you:
- Pick one or two brief measures that fit the client and their concerns
- Collect them regularly (for example, every session or once a month)
- Look at the scores together, alongside your clinical judgment
- Adjust treatment based on what you see
The measures might be symptom scales, simple 0–10 ratings or short wellbeing questionnaires. They do not replace your formulation or your relationship with the client. They add another piece of information to support decisions you are already making.
What the Research Says About Outcomes
Across different settings and modalities, research has consistently found that when therapists use measurement based care regularly, review scores with clients, and adjust treatment based on those scores, clients are more likely to show greater improvement and are less likely to quietly deteriorate in treatment.
You do not need a complex battery of tests to see benefits. Even a single, well-chosen measure, used consistently, can help you spot non-response and prevent silent deterioration.
Why Most Therapists Struggle to Implement MBC
Time, Admin and “Survey Fatigue”
Common barriers:
- Extra admin: printing, scoring, entering data into an EHR, trying to find old scores during a busy clinic day.
- Too many measures: long batteries that clients and therapists both tire of.
- Fragmented systems: measures sent from one app, stored in another, and rarely in front of you when you are actually in session.
When measurement feels bolted on rather than integrated, it’s natural to drop it when you get busy.
Concerns About Client Experience
Therapists also worry about:
- Turning sessions into tests: clients feeling judged by scores rather than heard as people.
- Triggering shame or defensiveness: especially if scores are not improving.
- Over-medicalizing: particularly in work that is more relational or exploratory.
These are real concerns, and they’re worth taking seriously. Most of them come down to how measures are chosen and introduced rather than whether measurement should happen at all.
Choosing Measures That Fit Your Practice
The best measures are ones you will actually use. Short, relevant and easy to explain usually beats “perfect but impractical.”
Brief Measures for Common Conditions (Depression, Anxiety, Trauma)
For many outpatient practices, a small set of brief measures covers a lot of ground. For example:
Depression
- PHQ-9 (9-item Patient Health Questionnaire): validated, fast to score, widely accepted by payers.
- Or a simple 0–10 rating of mood or “down days this week” if a full scale feels like too much.
When the diagnosis is recurrent moderate major depressive disorder, pair the PHQ-9 trend with a chart note that distinguishes single-episode MDD from F33.1 recurrent depression, rather than letting the score sit alone.
Anxiety
- GAD-7 (7-item Generalized Anxiety Disorder scale): covers worry, tension, and physical symptoms; paired well with PHQ-9.
- Or a 0–10 “anxiety in the past week” rating for clients who resist formal measures.
Trauma / PTSD
- PCL-5 (20-item PTSD Checklist for DSM-5): maps to DSM-5 symptom clusters; use where appropriate and safe. For trauma-focused cases where EMDR is part of the plan, review EMDR basics for therapists so SUD and VOC ratings complement, rather than replace, broader outcome tracking.
- Or targeted questions about nightmares, intrusions, avoidance and hyperarousal when a full checklist is too activating.
You might add other tools depending on your caseload (for example, substance use, eating concerns, OCD), but starting with one core area and a single, short measure is often enough to begin. For eating-disorder caseloads specifically, the EDE-Q and a binge/purge frequency log are the working measures; see measurement-based care for eating disorder therapy for how that cadence fits alongside technique selection and referral decisions.
When to Use Disorder-Specific vs General Wellbeing Scales
You do not need to choose between symptom and wellbeing measures. Each has a place.
Disorder-specific measures
- Best when you are treating a clearly defined problem (for example, panic disorder, PTSD).
- Help you see whether symptoms linked to that problem are changing as expected.
General wellbeing or functioning scales
- Capture broader changes in life satisfaction, relationships or work.
- Useful when clients have multiple issues or when your work is more integrative.
A simple approach:
- Pick one symptom measure linked to the main presenting problem.
- Pair it with one wellbeing or functioning measure if the client’s situation is complex.
You can always expand or refine your set of tools later as you find what fits your practice.
MBC tool comparison: which measure for which presentation
The table below summarizes the most-used validated measures in US outpatient practice. Picking from a small set you can administer reliably consistently outperforms cycling through many measures inconsistently.
| Measure | What it tracks | Items / time | Cadence | Best fit |
|---|---|---|---|---|
| PHQ-9 | Depression severity | 9 items / ~1 min | Every 2–4 sessions | Adjustment disorder, MDD, dysthymia, treatment monitoring |
| GAD-7 | Generalized anxiety | 7 items / ~1 min | Every 2–4 sessions | GAD, mixed anxiety presentations, often paired with PHQ-9 |
| PCL-5 | PTSD symptoms (DSM-5 aligned) | 20 items / ~5 min | At intake + every 6–8 sessions | PTSD intake assessment, monitoring across trauma-focused work |
| AUDIT | Alcohol use | 10 items / ~2 min | At intake + every 8 weeks | Substance-use screening, monitoring during sobriety work |
| ORS / SRS | General progress + alliance | 4 items each / 30 sec each | Every session | Integrative practice, alliance-focused work, brief therapy |
| WHO-5 | Wellbeing | 5 items / ~30 sec | Every 2–4 sessions | Recovery and wellness-focused work, integrative practice |
| DASS-21 | Depression / anxiety / stress combined | 21 items / ~3 min | Every 4 sessions | Mixed presentations where one combined measure beats stacking three |
The platform layer (Blueprint, Greenspace, Mirah, OWL Practice’s MBC module, plus EHR-embedded MBC in SimplePractice and TherapyNotes) handles the administration, reminder, scoring, and trend-tracking. The choice between platforms usually comes down to EHR integration, telehealth fit, and client-experience friction. The measure choice and the platform choice are independent decisions.
Deeper integration of measurement data into between-session client engagement is the focus of the upcoming Engagement Agent reference, which will cover the in-progress work that turns measurement-based care from a static dashboard into an active part of the therapeutic relationship.
Downloadable MBC starter pack
A printable one-page reference (the seven measures above with administration tips, the 4-week starter cadence, and a sample progress-note line for documenting score interpretation) is in the works for the next iteration of this guide. In the meantime, the table above can be reproduced on a single sheet using the column structure as written.
Simple MBC Workflows You Can Start This Month
Measurement based care becomes easier when built into routine rather than treated as an add-on.
Solo Practitioner Workflow
If you are in solo practice, aim for something you can sustain without extra staff.
A simple pattern:
- Choose 1–2 core measures you will use often (for example, a depression scale and a general wellbeing rating).
- Send them before sessions using secure online forms, or have clients complete them in the waiting room or at the start of telehealth calls.
- Review scores briefly in session: notice trends, ask what stands out to the client.
- Note key changes in your progress notes and, where relevant, your treatment plan. Mental health progress note templates and examples can help you capture these changes in a consistent, reusable format.
- Review every 4–8 weeks whether the chosen measures are still the right ones.
This can be done with basic tools (forms plus your EHR) or more integrated platforms that handle reminders and scoring.
Small Group Practice Workflow
In small group practices, the main challenges are consistency and communication.
Possible workflow:
- Agree on a core set of measures used across the practice for common presentations.
- Build them into your intake and first-session process so they become standard rather than optional.
- Use shared dashboards or simple reports to review patterns at clinician and practice level (for example, average change on a key scale).
- Include MBC in supervision: review cases where scores are not improving, and surface gains that clients might not recognize on their own.
Even a lightweight, shared approach can make a big difference to how aligned the practice feels and how you talk about outcomes with clients and referrers.
Larger Clinic or Organization Workflow
Larger organizations often have more resources, but also more complexity.
A sustainable approach might include:
- Embedding measures into the EHR so they are easy to administer and view alongside notes and treatment plans.
- Standardizing frequencies (for example, every session for high-acuity programs, monthly for longer-term work).
- Providing training and scripts for how to explain measures to clients, especially in diverse cultural contexts.
- Using aggregated data carefully for quality improvement, while protecting individual privacy and avoiding pressure that undermines clinical judgment.
Technology reduces friction, but change management matters just as much. MBC works best when therapists understand the rationale and have genuine input into how measurement is built into their workflow.
How to Talk About Measures with Clients
The way measures are introduced can shape how clients feel about them.
Framing Measures as a Tool, Not a Test
You might say, in your own words:
- “These short questionnaires help us notice changes over time that can be hard to see week to week.”
- “This isn’t a test you can pass or fail. It is just one way to track how things are going.”
- “Sometimes the numbers change before you feel it, or the other way around. Both are useful for us.”
Keep the focus on collaboration and curiosity, not evaluation or performance.
Using Scores in Session to Guide Conversation
Scores become more meaningful when you look at them together, for example:
- “Your score went up a bit this month. Does that match how things have felt?”
- “Your anxiety score is lower, but you’re still avoiding that situation. Let’s talk about that.”
- “We’re seeing a drop on the depression measure and you’re back at work three days a week. How does that feel for you?”
You can also invite clients to set their own “markers of progress” alongside formal measures, such as:
- Sleeping through the night most days
- Being able to attend a social event
- Feeling less dread on Sunday evenings
This keeps the work grounded in what matters to them.
Using Technology to Make MBC Sustainable
Technology can help with the time-consuming parts of MBC: sending measures, collecting responses, scoring and visualizing trends. The key is maintaining control of clinical decisions while offloading busywork.
If you are comparing specific ways to collect and review that data, the tools for tracking client progress guide maps the options therapists actually use.
Automated Reminders and Scoring
Useful features might include:
- Automatic invitations to complete measures before sessions (via email or SMS, within your privacy policies).
- Auto-scoring with clear alerts for significant changes or risk-related responses.
- Integration with your notes so key scores are visible while you are writing up sessions or treatment plans.
This reduces the chance that measures are forgotten on busy days and saves you from manual calculations.
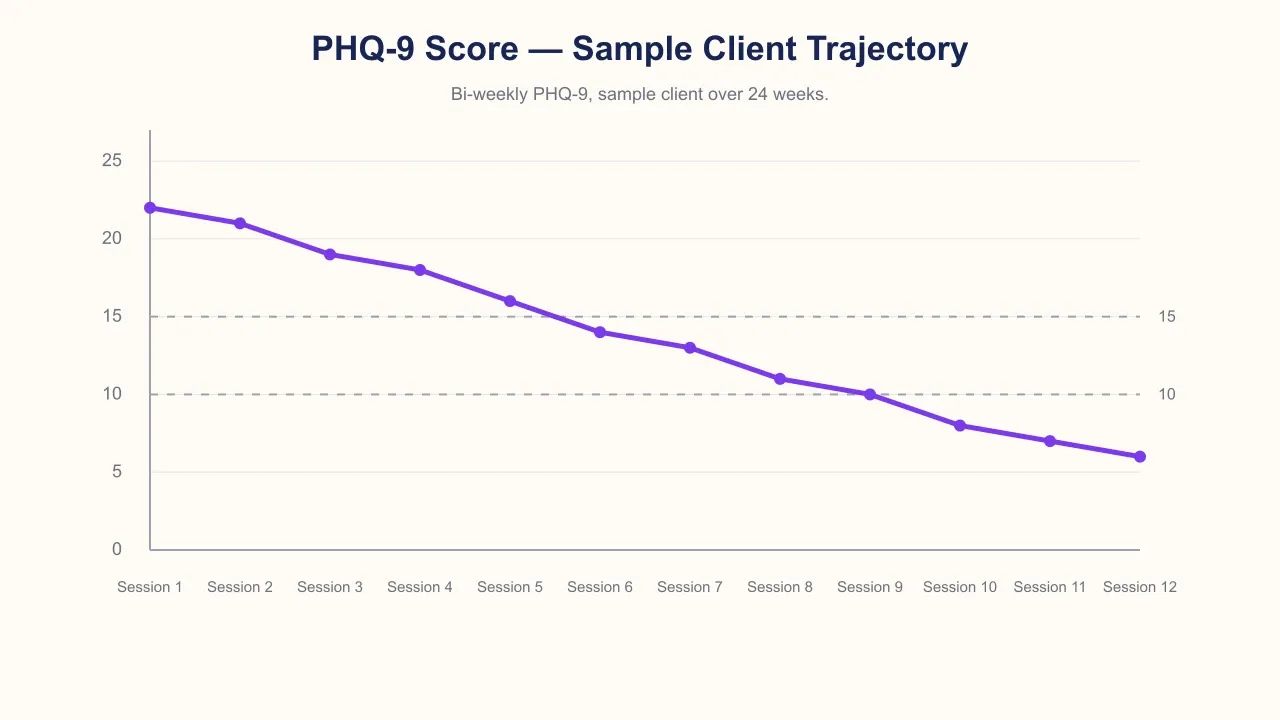
Visualizing Trends Over Time
Simple graphs can make progress tangible:
- Symptom scores over time, with notes on key events or treatment changes.
- Wellbeing ratings alongside life changes (for example, starting a new job, ending a relationship).
- Risk-related items highlighted when they shift significantly.
These visuals can help you and your clients:
- Notice small but meaningful improvements
- Catch early signs of deterioration
- Decide together when it might be time to change approach, intensify care or consider ending treatment
How Emosapien Can Embed Measures into Client Journeys
Emosapien is designed to support measurement based care for therapists without turning sessions into data entry.
In practice, that can look like:
- Embedding measures into intake and ongoing journeys: clients complete brief, tailored measures through secure digital touchpoints. You choose which ones to use and how often.
- Bringing scores into context: Emosapien can surface scores alongside your notes, treatment plans and key session themes, so you see not just the numbers but the story around them.
- Highlighting patterns and outliers: when a score changes significantly, Emosapien can flag it for your attention, helping you catch clients who are not improving or who might be at increased risk.
- Keeping privacy and ethics front and center: measures are handled within the same privacy-first framework as the rest of Emosapien, with clear data boundaries and no training of global models on your client data by default.
You keep control of which measures you use, how you interpret them and what you do next. Emosapien’s role is to reduce friction, link measurement to your existing treatment plan templates and outcomes tracking examples, and make it easier to build an AI-ready therapy practice step by step, without losing your clinical voice. For the operational picture of how this works in practice (auto-scoring, between-session scheduling, pre-session brief), see the companion piece on what changes when AI runs MBC for you.
Getting started
If you are just starting with measurement based care, you do not have to overhaul your practice overnight. You can:
- Choose one simple measure that fits your most common presentations
- Pilot a workflow with a handful of clients this month
- Gradually connect those measures to your treatment plans and progress notes
As your comfort and systems grow, you can bring in more structure, more nuance and more support from tools like Emosapien, always with the goal of making therapy more responsive and transparent, not more mechanical.
References
- American Psychological Association. (2019). Clinical Practice Guideline for the Treatment of Depression Across Three Age Cohorts. https://www.apa.org/depression-guideline
- American Psychological Association. (n.d.). Understanding Psychotherapy and How It Works. https://www.apa.org/topics/psychotherapy/understanding
- American Psychological Association. (2020). Measurement-based care: Using routine outcome monitoring to improve treatment. Monitor on Psychology. https://www.apa.org/monitor/2020/01/cover-trends-measurement-based-care