
Psychotherapy Notes Sample: Copy-Ready Examples and Variations
Outline
You finish a session, start writing, and catch yourself about to put a private process reflection into the shared progress note. That moment is the whole reason to keep two kinds of notes. This page gives you a complete, copy-ready psychotherapy notes sample plus a few practical variations, and draws a clear line between what belongs in your private notes and what belongs in the clinical record.
Disclaimer: This is general educational information, not legal advice. Requirements vary by jurisdiction, payer, and setting, so check your local rules and organizational policies. UK readers should also read the UK therapy notes and record keeping guide for HCPC/BPS and GDPR-aware practice notes, plus the BPS and HCPC expectations for UK psychologists when titles, chartered status, or register checks matter.
What psychotherapy notes are
Psychotherapy notes (sometimes called “process notes”) are your private clinical reflections about the session content and process. They often include hypotheses, impressions about transference/countertransference, therapist’s personal reminders, and sensitive process observations that support your thinking.
Under the HIPAA Privacy Rule, psychotherapy notes are defined separately from the rest of the record and given extra protection, which is why many settings treat them differently from standard clinical documentation. Practically, the biggest takeaway is this:
- Psychotherapy notes are for your own clinical use
- Progress notes are for the clinical record and care coordination
If you want familiar, structured formats for the clinical record, use our Mental Health Progress Note Templates and Examples for the side-by-side comparison of SOAP, DAP, and BIRP, all gathered under the clinical documentation hub.
If you need the writing workflow behind the clinical record, read how to write psychotherapy notes before adapting the samples below.
Psychotherapy notes vs progress notes
Here’s a clinician-friendly way to keep the separation clear.
| Category | Psychotherapy notes (process notes) | Progress notes (clinical record) |
|---|---|---|
| Primary purpose | Therapist’s private reflection and case formulation support | Document care provided, medical necessity, continuity, billing/audit needs |
| Tone | Reflective, hypothesis-driven, process-oriented | Objective, concise, structured, observable where possible |
| Typical content | Themes, therapist impressions, process dynamics, hypotheses, therapist reminders | Interventions used, client response, risks, symptoms, goals, plan, next steps |
| Sharing | Usually not routinely shared or used for billing | Often shared across care team and used for compliance/billing |
| ”Should include?” | Your clinical thinking that doesn’t belong in the record | What you did, why, how client responded, and what’s next |
Quick rule of thumb
- If it helps another clinician understand the care delivered (or supports billing/continuity), it belongs in a progress note.
- If it’s primarily your private process reflection (and not necessary for continuity of care), it’s a better fit for psychotherapy notes.
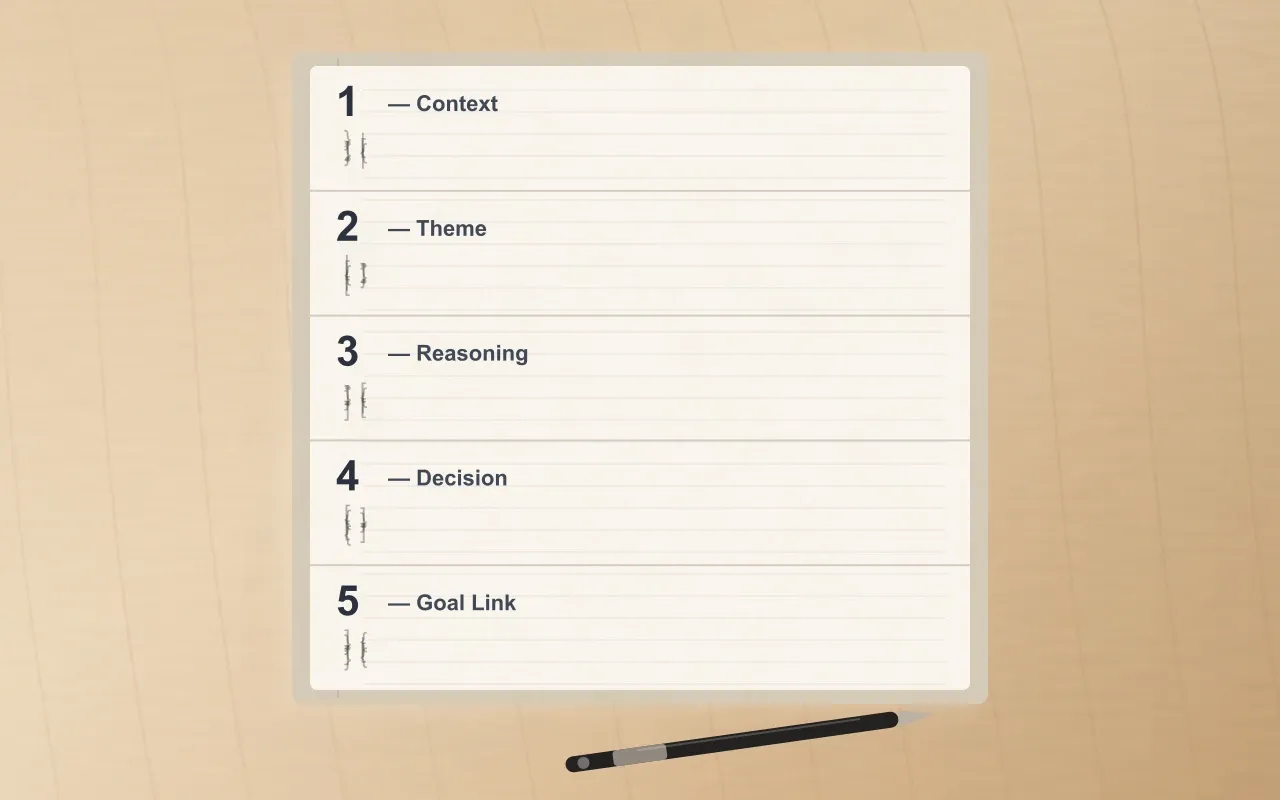
- 1 Context - what brought today's content to the surface: the prior session thread, a between-session event, a presenting affect.
- 2 Theme - the pattern or hypothesis you're tracking. Often a single clinical thread (transference, ambivalence, avoidance loop).
- 3 Reasoning - your private interpretive thinking. The work that doesn't belong in the shareable progress note.
- 4 Decision - what you chose to do or not do, in your own clinical voice. Includes shifts you considered but held back.
- 5 Goal Link - how this thread connects back to the active treatment goal, or signals that the goal needs to be revisited.
What typically belongs in psychotherapy notes
Common elements therapists include:
- Process observations (session flow, relational dynamics, ruptures/repairs)
- Clinical hypotheses and formulation updates
- Transference/countertransference reflections (as relevant)
- Therapist reminders for next session (questions to explore, patterns to track)
- Sensitive content not required for the clinical record (written respectfully, without unnecessary detail)
What typically does not belong in psychotherapy notes (or doesn’t need detail there):
- Billing justification, administrative details, routine symptoms checklisting
- Full narrative replay of trauma content (often unnecessary and increases documentation risk)
- Identifiers or unnecessary specifics (keep it minimal either way)
For aligning notes to treatment direction, keep goals measurable and consistent across your documentation, so session reflections connect back to the active plan instead of drifting.
Psychotherapy notes sample
Below is a sample you can copy, paste, and adapt. It uses no real client data.
Sample variations
Concise version (8–10 lines)
A shorter version for high-volume weeks.
Sample psychotherapy notes (CBT-oriented process emphasis)
Sample psychotherapy notes (relational / EFT-style process emphasis)
Common mistakes to avoid (clarity and boundaries)
These are practical issues therapists run into, especially when busy:
- Blurring psychotherapy notes and progress notes (mixing reflective process content into the clinical record)
- Writing too much detail (long narratives that don’t improve care continuity)
- Using loaded language instead of clinical, respectful phrasing (even in private notes, keep professionalism)
- Capturing identifiers unnecessarily (use initials/ID, keep sensitive specifics minimal)
- Skipping the “next intention” (a one-line intention keeps your thinking organized without over-documenting)
If your upstream documentation is messy, it can leak into both progress notes and psychotherapy notes. Clean intake data helps keep both cleaner from the start.
FAQ
What is the difference between psychotherapy notes and progress notes?
Psychotherapy notes are your private process reflections (themes, hypotheses, relational dynamics). Progress notes document care delivered in the clinical record (interventions, client response, risks, plan). For templates and formats like SOAP/DAP/BIRP, use the Mental Health Progress Note Templates and Examples guide linked above.
Can I use this sample as-is?
Yes, the sample above is designed to be copy-ready, but you should adapt it to your setting, documentation policy, and local requirements.
Should psychotherapy notes include interventions and homework?
Often, interventions and homework belong in progress notes because they support continuity of care. In psychotherapy notes, you might include a brief therapist reminder (for example, “consider exposure ladder framing next time”) without duplicating the full plan.
Are psychotherapy progress notes samples the same thing as psychotherapy notes?
Not usually. “Psychotherapy progress notes samples” typically refer to progress notes written after psychotherapy sessions, often using structures like SOAP/DAP/BIRP. Psychotherapy notes (process notes) are more reflective and private.
Where can I find free sample psychotherapy progress notes?
If you’re looking for free sample psychotherapy progress notes, start with structured examples and formats like SOAP/DAP/BIRP, then tailor to your clinical style. The Mental Health Progress Note Templates and Examples guide linked above is the fastest next step.
Conclusion (key takeaways)
- A psychotherapy notes sample should be reflective, process-focused, and minimal - aimed at supporting your clinical thinking.
- Keep psychotherapy notes and progress notes clearly separated to reduce confusion and improve workflow consistency.
- Use progress note structures (SOAP/DAP/BIRP) for the clinical record; keep process reflections in psychotherapy notes.
- Avoid over-detailing, keep identifiers minimal, and write in professional clinical language.
- If you want a quicker starting point, Emosapien can draft session notes and summaries for therapist review, while you stay in control.
If you’d like to speed up documentation without losing your voice, try Emosapien to generate structured notes faster and reduce admin time, then edit and finalize in minutes. If you’d rather have an AI co-therapist draft these notes while you focus on the client, see Emosapien’s AI Clinical Notes.
References
- U.S. Department of Health & Human Services. HIPAA Privacy Rule guidance on psychotherapy notes.
- U.S. Government Publishing Office. 45 CFR 164.501 — HIPAA definitions.
- American Psychological Association. Record Keeping Guidelines.